In our patriarchal society, for anything good that a child does, inadvertently credit goes to father and for the opposite, the mother is held responsible.
My parents for once, never in their worst of nightmares would have realized that they might have passed on a defective gene responsible for the devastating genetic progressive muscular disorder to us twins. For all we know it could have been a sporadic mutation in our genes at the time of our inception in the womb.
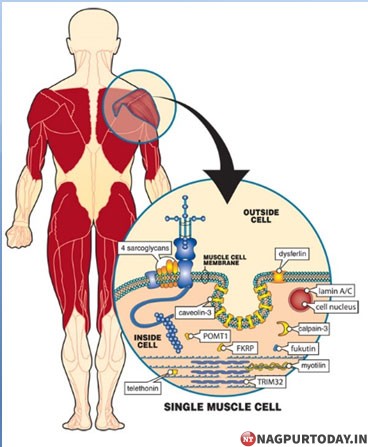
We are suffering from Limb Girdle Muscular Dystrophy subtype R2, i.e. Dysferlinopathy, a form of Muscular Dystrophy (MD) with adult onset of symptoms, which include : Walking with a “waddling” gait because of weakness of the hip and leg muscles; Difficulty getting out of chairs, rising from a toilet seat, or climbing stairs due to weak pelvic girdle musculature; Trouble in reaching over the head, holding the arms outstretched, or carrying heavy objects due to weakness in the shoulder area. LGMD can be inherited in one of two basic ways that are known as the autosomal dominant pattern and the autosomal recessive pattern. The word “autosomal” means that the genes involved are not on the X or Y chromosome and, therefore, are passed on from men, women, or both
In a glaring instance in Kolkata, a mother to a DMD (Duchenne Muscular Dystrophy) child had to end her life due to constant distress, helplessness faced by her DMD son and lack of awareness and proper education about the disease. This is such an unfortunate incident and a shame to our society where we worship the likes of Goddess Durga and talk about women empowerment and child education.
How could a mother, who is the epitome of selflessness and love, be held responsible for a disease which she unknowingly passed on.
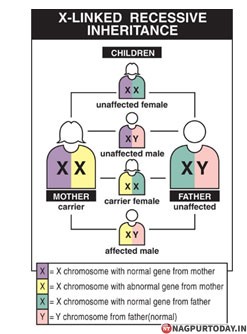
DMD is inherited in an X-linked pattern because the gene that can carry a DMD-causing mutation is on the X chromosome. Every boy inherits an X chromosome from his mother and a Y chromosome from his father, which is what makes him male. Girls get two X chromosomes, one from each parent.
Each son born to a woman with a dystrophin mutation on one of her two X chromosomes has a 50 percent chance of inheriting the flawed gene and having DMD. Each of her daughters has a 50 percent chance of inheriting the mutation and being a carrier. Carriers may not have any disease symptoms but can have a child with the mutation or the disease. DMD carriers are at risk for cardiomyopathy

A man with DMD cannot pass the flawed gene to his sons because he gives a son a Y chromosome, not an X. But he will certainly pass it to his daughters, because each daughter inherits her father’s only X chromosome. They will then be carriers, and each of their sons will have a 50 percent chance of developing the disease and so on.
Usually, girls do not experience the full effects of DMD the way boys do, although they still have symptoms of muscle weakness. A minority of females with the mutation, called manifesting carriers, have some signs and symptoms of DMD. Regular strength evaluations and close cardiac monitoring is needed to manage any symptoms that may arise.
Onset of DMD is as early as 2 years, a tender age for a child to flourish, when this debilitating disease starts showing its symptoms and worsens with age. A preschooler with DMD may seem clumsy and fall often. Parents also may note that children have trouble climbing stairs, getting up from the floor, or running. When arising from the floor, affected boys may use hand support to push themselves to an upright position. By school age, children may walk on their toes or the balls of their feet with a slightly waddling gait and fall frequently. To try to keep their balance, they may stick out their bellies and pull back their shoulders. Children also have difficulty raising their arms. In the teen years, activities involving the arms, legs, or trunk may require assistance or mechanical support such as wheelchairs, calipers, etc.
Patients with DMD often lose out to disease in their late teens or 20s from respiratory insufficiency or cardiomyopathy; only a few DMD patients survive beyond the third decade. It is critical that babies with these conditions are screened so they can receive an early diagnosis in order to get the life-changing and lifesaving care they need as soon as possible.
Every other week we witness a sharp, intelligent DMD child, who could have become a pride of our country, losing out to this dreadful disease.
Muscular dystrophy is fast becoming an alarming situation in our society. Instead of taking drastic steps to contain the disease and provide proper management and support services, our Government is still turning deaf ears to our requests. Muscular Dystrophy has NO CURE in the world. Many doctors portray a very grim picture to the family with MD patients. With adequate rehabilitation including physiotherapy, healthy diet, dietary supplements and a positive mindset, we can go a long way to preserve muscle mass and strength.
A lot of money is wasted on alternative therapies which hardly provide any relief and a major chunk of family’s income is withered away which could have been well spent on upkeep , care and management of the disease. Government needs to issue clear and crisp directives to doctors who need to caution patients against any mala fide practices being run by quacks who claim to better the life of patients. On compassionate grounds, doctors must provide empathy to family who is already in shock at diagnosis of MD.
We at Muscular Dystrophy Patient’s Welfare Society are a strong patient advocacy group that re-enforces belief in mothers and families who are the pillars of support to MD patients. Our members are well integrated with other NGOs like PPMD, IAMD, AMDA, TMDA, etc to proactively build up hope and belief in emerging therapeutic treatments which have the potential to offer relief and arrest the decline of MD. To approach scientific community for clinical studies, Government for policy decisions and organisations for raising funds to support clinical studies, we are in process of forming National registries for MD and all MD afflicts can register with us at undermentioned contact numbers.
Instead of ostracizing and isolating the families with Muscular Dystrophy patients, we must develop an all- inclusive ecosystem to encourage and provide emotional and physical support to the family and patients. Health is a state subject. We expect our government to form a high level committee dedicated to work towards providing benefits and relief to family who silently suffers at the hands of this atrocious disorder. To fulfil high costs towards maintenance of this disease, many have drained their resources including selling off their lands, giving up their careers, taking loans and are eyeing eagerly towards any financial support from government.
This committee must develop a team of scientists to cohesively works towards providing treatment and bringing “Bridging trials” of successful drugs in phase 3 for this disorder. All types of MD must be listed as severe disability in National Health Mission as soon as possible. This disease with due respect to cancer survivors is worse than cancer due to its progressive nature which renders the patient helpless with as trivial an activity as scratching due to mosquito bite, having our favourite icecream, drinking glass of water when thirsty, playing outdoors, socializing with friends and family and much more. Insurance companies must come forward to cover the monumental costs of treatment and disease management. First and foremost free genetic testing must be provided alongwith necessary Genetic counselling to diagnose the disease and contain its spread.
Written by Gitika Khanna +91 9818227215
You may reach Ajit Sinha at +91 8208570955, Mangesh Pedamkar at +91 9664888111